


COVID-19 Vaccines
Not Safe and Effective

This is a 12/27/22 Thread converted from Twitter.
It has been two years since the EUA was issued for the COVID-19 Vaccines. We have been told ad nauseam they are “safe & effective”, but is that truly the case? There have been hundreds of studies conducted that tell a different story, a story that is being suppressed and I aim to go through the evidence and hopefully change your mind if you were still under the illusion that these injections are a benefit to anyone.
First, let’s state some facts that are now undeniable with the benefit of hindsight.
The Infection Fatality Rate for Covid is a worldwide average of 0.23%.
https://apps.who.int/iris/bitstream/handle/10665/340124/PMC7947934.pdf?sequence=1&isAllowed=y
Risk is highly age-stratified. If you are under 70 w/o major co-morbidities you have a 99% chance of survival. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9613797/
The vast majority of covid deaths were experienced by people over 75 and with multiple co-morbidities like obesity or diabetes. https://www.statista.com/statistics/1191568/reported-deaths-from-covid-by-age-us/
Children are not in danger from covid and the major have natural immunity. They were never at risk personally or at risk to spread it widely.
“Asymptomatic” spread was and never has been a driving factor in infectious disease outbreaks. It was a lie with no evidence and used to justify lockdowns and other ghastly world-destroying policies.
One could argue that given these facts alone, the need for a vaccine should have been out of the question. Nonetheless, a vaccine is experimental and injected into 5 billion people with no long-term studies. That would be logical if we didn’t live in a world that has been so thoroughly corrupted.
Keep in mind that there are many others ways to treat covid that are genuinely safe and effective. It’s just that they have all been demonized in lockstep, on a worldwide scale. The fact that this was achieved so successfully should send shivers down your spine.
The only solution given was the vaccines. No other options. They were touted as 95% effective based on the clinical trials. Every news organization dutifully reported those fraudulent numbers. This has been shown in the data that was released by Pfizer and only after they were sued to do so.

I won’t go into the motives of those who have so fervently pushed these vaccines, that is for another thread. I am going to focus on what the science says and present enough evidence that anyone with a brain could come to the conclusion that the risk posed by these “vaccines” is far greater than the risk posed by the virus.
In fact, the “vaccines” are the true public health crisis that is just now coming into focus thanks to researchers publishing data contrary to the orthodoxy being imposed on the world. As dark as this subject matter is given the evidence, this should provide some hope that there are people who care about humanity and won’t stand by idly while sociopaths seek to destroy it.
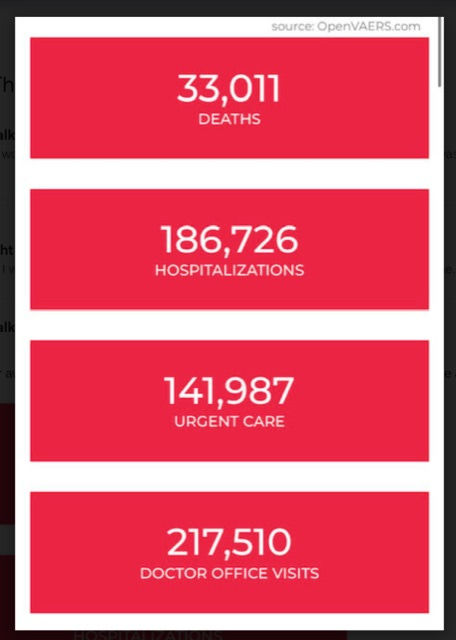
First, let’s look at VAERS as shown today, and keep in mind VAERS is highly underreported so these numbers are very likely to be higher by orders of magnitude.
Does this look “Safe and Effective”?
These numbers are also consistent with Europes reporting on adverse side effects as well as other governmental sources of data. Don’t let people gaslight you when it comes to reported outcomes, that is a tactic of low-information tyrants. A false report on VAERS is punishable with a prison sentence and most reports are inputted by hospital staff and validated by the CDC. The next section will offer several scientific studies with a brief overview of their conclusions. I have linked to all studies if you feel the need to verify the claims.
The Science
Serious Adverse Events of Special Interest Following mRNA Vaccination in Randomized Trials https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4125239
“The excess risk of serious adverse events of special interest surpassed the risk reduction for COVID-19 hospitalization relative to the placebo group in both Pfizer and Moderna trials “
“Increased emergency cardiovascular events among the under-40 population in Israel during vaccine rollout and third COVID-19 wave”
https://www.nature.com/articles/s41598-022-10928-z
“the findings raise concerns regarding vaccine-induced undetected severe cardiovascular side-effects and underscore the already established causal relationship between vaccines and myocarditis, a frequent cause of unexpected cardiac arrest in young individuals.’
“Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs”https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9012513/
A thorough review of the evidence, look at these conclusions. NOT SAFE AND EFFECTIVE.
“In this paper, we call attention to three very important aspects of the safety profile of these vaccinations. First is the extensively documented subversion of innate immunity, primarily via suppression of IFN-α and its associated signaling cascade.”
“This suppression will have a wide range of consequences, not the least of which include the reactivation of latent viral infections and the reduced ability to effectively combat future infections.”
“Second is the dysregulation of the system for both preventing and detecting genetically driven malignant transformation within cells and the consequent potential for vaccination to promote those transformations.”
“Third, mRNA vaccination potentially disrupts intracellular communication carried out by exosomes and induces cells taking up spike glycoprotein mRNA to produce high levels of spike-glycoprotein-carrying exosomes, with potentially serious inflammatory consequences.”
“Should any of these potentials be fully realized, the impact on billions of people around the world could be enormous and could contribute to both the short-term and long-term disease burden our health care system faces.”
Potential antigenic cross-reactivity between SARS-CoV-2 and human tissue with a possible link to an increase in autoimmune diseases
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7246018/
“The promotion and implementation of such an aggressive “immune passport” program worldwide in the absence of thorough and meticulous safety studies may exact a monumental cost on humanity in the form of another epidemic, this time a rising tide of increased autoimmune diseases and the years of suffering that come with them.”
“Myocarditis Following Immunization With mRNA COVID-19 Vaccines in Members of the US Military”https://jamanetwork.com/journals/jamacardiology/fullarticle/2781601
“In this case series of 23 male patients, including 22 previously healthy military members, myocarditis was identified within 4 days of receipt of a COVID-19 vaccine. For most patients (n = 20), the diagnosis was made after the second dose of mRNA COVID-19 vaccine”
“COVID-19 vaccine boosters for young adults: a risk-benefit assessment and ethical analysis of mandate policies at universities “
https://jme.bmj.com/content/early/2022/12/05/jme-2022-108449
Our estimate shows that university COVID-19 vaccine mandates are likely to cause net expected harms to young healthy adults—for each hospitalisation averted we estimate approximately 18.5 SAEs and 1430–4626 disruptions of daily activities—that is not outweighed by a proportionate public health benefit. Serious COVID-19 vaccine-associated harms are not adequately compensated for by current US vaccine injury systems.
“Surveillance of COVID-19 vaccine safety among elderly persons aged 65 years and older”https://www.sciencedirect.com/science/article/pii/S0264410X22014931
“Four outcomes met the threshold for a statistical signal following BNT162b2 vaccination including pulmonary embolism, acute myocardial infarction, disseminated intravascular coagulation and immune thrombocytopenia”
“Autopsy-based histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination”
https://link.springer.com/article/10.1007/s00392-022-02129-5
“In general, a causal link between myocarditis and anti-SARS-CoV-2 vaccination is supported by several considerations:
(A) a close temporal relation to vaccination; all cases were found dead within one week after vaccination
(B) absence of any other significant pre-existing heart disease, especially ischaemic heart disease or cardiomyopathy
(C) negative testing for potential myocarditis-causing infectious agents,
(D) presence of a peculiar CD4 predominant T-cell infiltrates, suggesting an immune-mediated mechanism. The latter criterion is supported by the demonstration of a phenotypically identical T-cell infiltrate at the deltoidal injection site in one of the cases.”
“Myocarditis After BNT162b2 and mRNA-1273 Vaccination”
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.121.055913
“The temporal association between receiving an mRNA-based COVID-19 vaccine and the development of myocarditis is notable. Trials that tested the BNT162b2 and mRNA-1273 vaccines showed that systemic reactogenicity more often occurred after dose 2 and generally within 48 hours after vaccination.
“On average, our patients presented with symptoms of acute myocarditis 3 days after the second injection, and in 5 out of 8 patients fever appeared a day before, supporting the hypothesis that myocarditis could be an mRNA vaccine-related adverse reactions”
“Curing the pandemic of misinformation on COVID-19 mRNA vaccines through real evidence-based medicine – Part 1”
https://insulinresistance.org/index.php/jir/article/view/71
Conclusion: It cannot be said that the consent to receive these agents were fully informed, as is required ethically and legally. A pause and reappraisal of global vaccination policies for COVID-19 are long overdue.
“FDA oversight of clinical trials is “grossly inadequate,” say experts”
https://www.bmj.com/content/379/bmj.o2628
“This lack of oversight was not an isolated case, The BMJ has learned. Regulatory documents show that only nine out of 153 Pfizer trial sites1 were subject to FDA inspection before licensing the mRNA vaccine. Similarly, only 10 out of 99 Moderna trial sites2 and five of 73 Remdesivir trial sites3 were inspected.”
“Vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis post COVID-19 vaccination; a systematic review”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8330139/
“Healthcare providers should be familiar with the clinical presentations, pathophysiology, diagnostic criteria, and management consideration of this rare but severe and potentially fatal complication of the COVID-19 vaccination. Early diagnosis and quick initiation of the treatment may help to provide patients with a more favorable neurological outcome.”
“Blood Pressure Increase following COVID-19 Vaccination: A Systematic Overview and Meta-Analysis”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9147472/
“Overall, included studies accrued 357,387 subjects with 13,444 events of abnormal or increased BP. The pooled proportions of abnormal/increased BP or stage III hypertension recorded following vaccination (3.20% and 0.6%, respectively) showed that this event should not be considered sporadic”
I have provided 10 pieces of evidence, all with conclusions that fly in the face of current covid cult orthodoxy. This is but a small sample size and with every day that passes, more data and analysis streams that contradict what every media outlet, academic institution, governmental body, and major corporation spews forth in unison.
That alone should be enough to raise the specter of extreme skepticism yet the covid drumbeat continues. More boosters, and more mRNA injections for everything are being planned. We must reject these agendas because the future of the human species may depend on them.
Thanks for reading and if you’ve found this helpful give me a follow me on Twitter here @JoshWalkos and subscribe to this substack if you haven’t already for more to come.